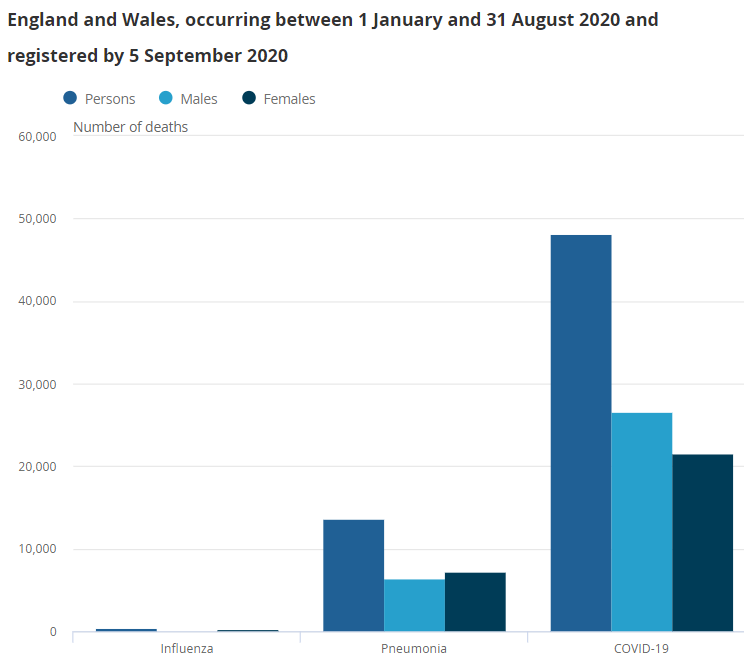
I think the government may have arrived at a number (or are close to it) that they think is acceptable…The first 7 months of last year we were at ~250 deaths/week. We’re at about 130 (as you say) now - at the peak of the latest wave. Initially, we will likely need to settle somewhere (possibly quite significantly) north of where the deaths from flu are on the plot below. I am hopeful that by spring the weekly death toll should be well below that of pneumonia, though likely still above flu and that we should be approaching some sort of “as you were” pre-covid normalcy. The key for me is making sure we carry on monitoring the variants (trough sequencing) as they are coming up and have a “cocktail” vaccine each year.
Very much but the I find the lack of attention to that fact pretty deafening.
Key metric for UK government is not to see the NHS struggle. Screw staff morale, welfare etc. Provided the numbers in hospital can’t be used to illustrate the funding and resource problems As a result of government policy then any number of deaths is fine.
It is now hard for me to see how this continues - Omicron has spread and is spreading so quickly that in practical terms, virtually the entire global population will be exposed to it by the end of February. That is not a condition that is favourable to producing a wide range of variants. Any mutation will need to have an extreme antibody breakthrough property to have a chance to survive, because by about the first week of March, there will be no pool to leap to - other horrific variants may mutate, emerge in the massive spike we will see to start 2022, and infect very few people before disappearing.
This is what I find interesting. So variants exclude infection by other variants? So you can’t have Delta and Omicron simultaneously, for example? Why is that?
I think excess deaths are useful now that we’ve had 6 months of most restrictions being lifted here in England. I’m on my phone so can’t open the raw data but November saw 1700 excess deaths a week (Statista) or 242 excess deaths a day. Is that acceptable? If yes, then you have to ask the question, could we be having a good COVID year? Or a good Flu year? If course those both could be true so saying “ok 242 additional daily deaths is acceptable” but those figures could in reality be astronomically higher next winter.
Things are probably still too precarious to let the leash off COVID.
The next step of getting back to normal is the one that is in all the intro epidemiology text books that we should have been employing from March 2020 - widespread rapid and effective testing with targeted isolation for people who are contagious with a test to exit requirement. The rapid antigen tests do a really good job of that, albeit not perfect. However, the people focusing in on the limitations of their ability to identify contagiousness are then throwing their hands up and just saying “you do you.” It’s madness.
For this approach to be employed the production of the tests has to go up by orders of magnitude, and so I think a big reason it is not being advocated is due to logistics. I think there is concern that if we forced companies like Abbott to undertake the efforts to scale up tot hat degree by the time they were the wave would be over and we’d be back where we were in the summer with Abbott having tens of millions of tests (in this case more) warehoused that no one wanted to buy and ultimately having to destroy them.
I don’t believe they do exclude infection per se, I don’t think any evidence of that has been found. But critically, we also have yet to encounter a variant that has complete evasion - our developed immune response to any given variant works to some degree on all known variants, with time since infection (or vaccination) appearing to be the key variable.
The effect is to squeeze out the window of opportunity for any slower variant. Delta and Omicron can co-exist (in theory) in an individual host, but if from the moment of infection Omicron outcompetes Delta in that host, the immune response triggered by Omicron is working against Delta as well. The probability of that host then infecting anyone else is much, much higher for Omicron than for Delta. Iterated over a population, Omicron will just get to so many that Delta will be starved out - and Delta hasn’t shown any particular propensity for re-infection, where Omicron has.
Omicron is in effect an extreme selective pressure on all potential new variants - only the ability to spread even faster or to infect a recently-infected Omicron host will allow a new variant to survive and reproduce. At some point as well, the number of generations may matter as well as the sheer number of reproductions. Omicron is going to reproduce an astronomical number of times, but the chain of generations will be shorter than Delta which has been running along for nearly a year.
Some worrisome data coming out of Massachusetts, which has done better than much of the US in prior waves. Hospitalization and ICU usage are all climbing dramatically, approaching the levels of one year ago. Showing a very different slope than South Africa or the UK, much more like Denmark.
Fair play to South Africa. They sort of fucked up with Beta but they could be on to a winner with Omicron. It just might be our way out of this pandemic.
I hope you’re right. Just looking at the data again.
UK 2nd wave peaked at 88.9 cases per 100k. We’re now at 232.7 cases per 100k and the curve is showing no signs of flattening out yet. It’s climbed from 72 cases per 100k to where we are now in less than 3 weeks. That’s crazy fast.
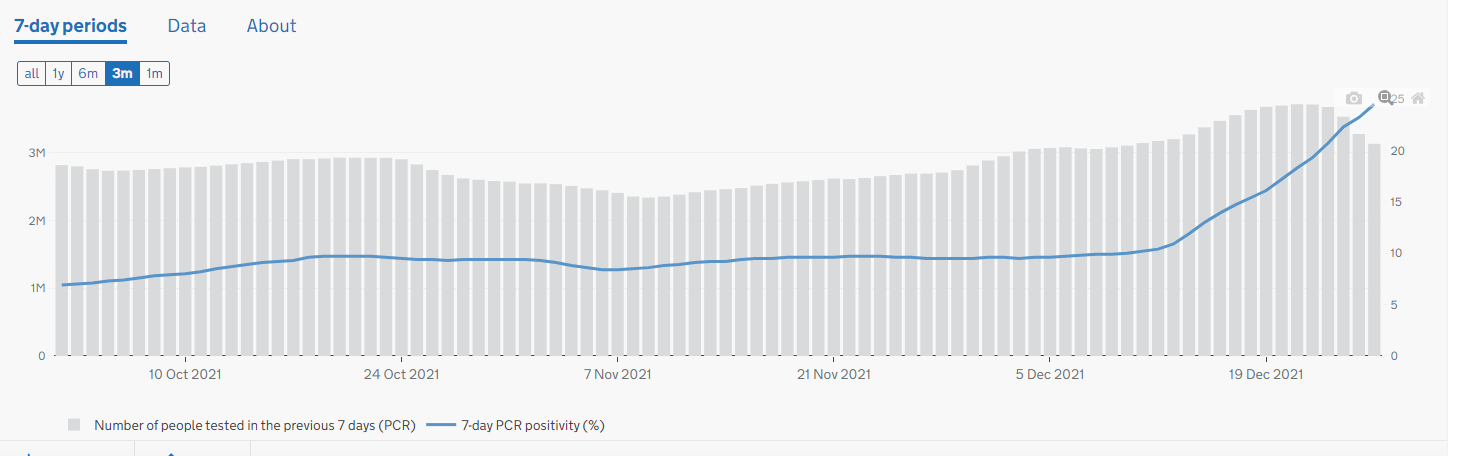
Despite the UK’s phenomenal rate of testing, it is pretty clear that those numbers are understated. UK positivity is soaring, which indicates the underlying number of cases is far higher.
Here, we have restricted access to PCR tests, essentially rationing them to essential sectors and directly-at-risk populations, and yet we are still testing at near capacity, and still seeing a positivity approaching 30%. Chillingly, the Ontario government decided to simply stop reporting the number of cases in schools and child care.
Interesting development here:
Omicron is now dominant in our country (65% vs. 35% for the delta variant).
We are still at an all-time high in terms of new cases, with maybe more to follow (currently 20k each day, for a population of eight millions, but I know for a fact that it’s very difficult currently to get tested right now, so the real numbers are probably higher than that). Some experts predict that half of the population will have been contaminated by omicron before the end of this month.
But on the other hand, the rate of new hospitalisations is steadily sinking. We had a peak of 125 hospitalisations each day three weeks ago, when delta was still dominant. Now, we are at more or less 70 each day. The number of people on intensive stations with covid-19 is roughly 37% of all available ones, with a current total occupation rate of 80%. It’s high, but manageable for the time being. The number of deaths is also steadily going back. We had a total of 90 deaths last week, which brings us back to where we were in november, with a clear trend to become even less. I wonder if that has to do with better ways to treat patients as well.
The biggest problem right now is that a lot of treating personnel in hospitals get the new variant and have to be withdrawn for quarantine, leaving the hospitals with a lack of personnel, and thus under a lot of stress. Same for other parts of the economy. That’s why the authorities have decided to shorten the time of quarantine from ten to seven days from today on.
My assumption here is that there will now always be a pool of COVID19 variants circulating. The discrepancies in who gets what vaccine, when and how often, will mean that there will (potentially) always be pockets within the global population where the virus will have a chance to incubate/circulate and flare up.
Just as Omicron is able to get through the double vaccinated ( and some boosted) individuals, is there any reason other variants could not arise with a similar profile from the vast numbers that will be infected by the end of Feb/Mar?
Your premise may well be flawed though. Why would there always be a pool of variants circulating? That is not necessarily the case. A variant only exists it is has some competitive advantage, which may or may not be localized. Omicron has created extreme selective pressure for all other variants - creating the possibility of a monoculture.
As I noted above, the vaccine has become more or less irrelevant to the distribution of the virus, though it still has real implications for the observed virulence. WHO is not ready for the politics of saying so, but with the observed breakthrough rate of Omicron for even 3 doses, vaccination with the current vaccines is off the table as a suppression tool.
As for the possibility that another variant could emerge - yes. It could happen. However, that runs to the extreme selection logic. The only variants that can survive in the Omicron spike are those that are at least as infectious as Omicron. Any other advantage or variation is irrelevant to the competition. If you were trying to produce conditions for the constant emergence of new variants, you would not want the whole world to be infected in a matter of months - ideally, there would be pockets of population that had prior antibodies fade, etc., and then the variants could travel in waves. It doesn’t look like we are going to see that. Similarly, the number of generations appears to have an influence on the likelihood of mutation - the same numbers spread over a year are more likely to produce deviations from the original pattern than over just a couple of months.
A successful variant is still possible, but not nearly as likely - whereas the emergence of something like Delta from Beta was virtually certain.
My hope is that by next Christmas this will be more endemic, and we will be living with it, possibly by taking a regular booster shot like the flu, or maybe a pill. There will still be deaths, but sort of like the flu. Still will kill thousands each year, so vigilance needed, but it will be the sort of thing we live with without too much disruption.
How we get there will have left a lot to be desired, with government missteps and a sizable segment of the populace prone to misinformation.
On that last point, I will be going to a funeral on Saturday of a friend. 50 yrs old. Educated man, business owner, employees, money, etc. His wife very strongly anti-vaccination and him somewhat… though to what degree he went along with her, or genuinely was himself anti-vaccination it’s hard for me to tell.
Anyway, two lovely kids, a girl and a boy, early teens, will be at their dad’s funeral on Saturday, to say nothing of the wife left behind. It’s all such a waste. He died on Christmas Day and that will never be the same again for his family. His wife is angry and trying to turn her attention on the hospital. He had excellent care, but as everyone in the medical field knows, intensive care is full of unvaccinated people. It’s tragic.
There are two elements to this though. One is inherent - how well does it infect the system. The other is contextual and based on our immune response to it. Omicron appears to have advantages in both aspects, but is also definitely taking advantage of the waning immunity of those who were previously thought to be fully vaxxed. Infection with Omicron appears to provide protection against the other strains we’ve seen so far, but doesnt mean it will against any of the variants it rampant spread is giving opportunity to now. If one of those emerges that has better immune escape then we’ll see another wave with yet another variant even if it is inherently less infectious than Omicron.
One of the things I keep seeing is that the relationship between cases and bad clinical outcomes has gone, almost positioning it as if cases are no longer an important metric. That is unfortunately not true. Sure, we cannot look at case numbers now and compare them to those in previous waves as a measure of the seriousness of the situation, we just need to recalibrate out thinking to understand what the new ratio is as cases are still going to be the driving factor on creating bad clinical and community outcomes.
Agreed - it has to be more infectious in one dimension or another, the ability to re-infect, the ability to infect vaccinated populations, or the simply the ability to infect more readily. It could happen, but the conditions are not as ideal as I would say there were prior to Omicron.